Case SummaryA 66 year old gentleman, non-smoker,
with diabetes, hypertension and hypercholesterolemia presented with unstable
angina. He had past history of triple vessel disease with coronary stenting
done in another hospital in 1995, the details of which was unknown. Coronary
angiogram revealed severe mid LAD in stent restenosis (ISR), severe proximal
LCX in stent restenosis and distal to stent another subtotal occlusion,
whereas proximal RCA was near totally occluded (
Movie 1,
Movie 2,
Movie 3). The mid LAD lesion was first treated in last session smoothly
but subsequent attempts to open LCX ISR failed despite repeated use of high
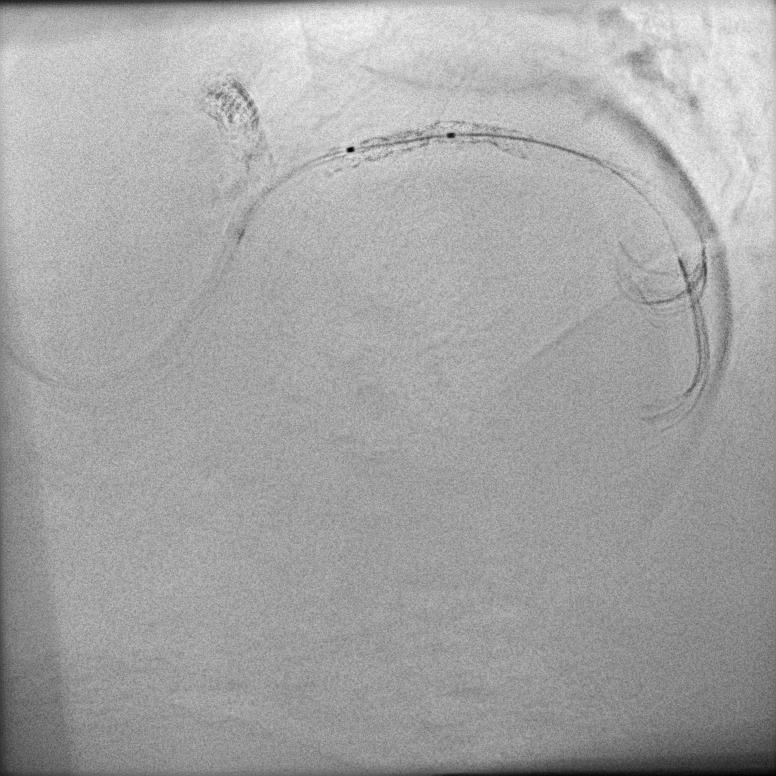
pressure noncompliant balloons. IVUS showed circumferential calcium and
under-expansion of previous stent (
Movie 4,
Figure 1) despite it failed to advance distally.
ProcedureLCX was reattempted 3 months later (
Movie 5,
Movie 6).
6F EBU 3.5 guide was used. LCX to OM was wired with
Fielder XT supported with Finecross microcatheter (
Movie 7). The undilatable pLCX segment was again POBA with multiple high
pressure noncompliant balloons including Angioscult 2.5x15mm (26atm), OPN
NC 2.5x10 (40atm), NC Emerge 3x12mm (26atm), OPN NC 3x10mm (40atm),
eventually the distal segment of the old stent opened up but not the
proximal stent part (
Movie 8). Therefore, it was decided for rotablation with 1.5 burr then upsize
to 1.75burr. However, it still failed to dilate the lesion. Afterwards, we
retried POBA with OPN NC 3x10mm and the lesion finally yielded at high
pressure (37.5atm) which was confirmed with IVUS (
Movie 9). In view of small dLCX, it was decided to stent into OM with
Ultimaster 2.5x28m overlapped with Ultimaster 3x33mm proximally. Subsequent
angiographic result was excellent (
Movie 10,
Movie 11).
{kind=link}